Longer Term All-Cause and Cardiovascular Mortality With Intensive Blood Pressure Control
A Secondary Analysis of a Randomized Clinical Trial
Longer term all-cause/CVD mortality
We assessed all-cause1 and cardiovascular disease2 (CVD) mortality post-trial via the US National Death Index (NDI) from 2016-2020 (Jaeger et al. 2022).
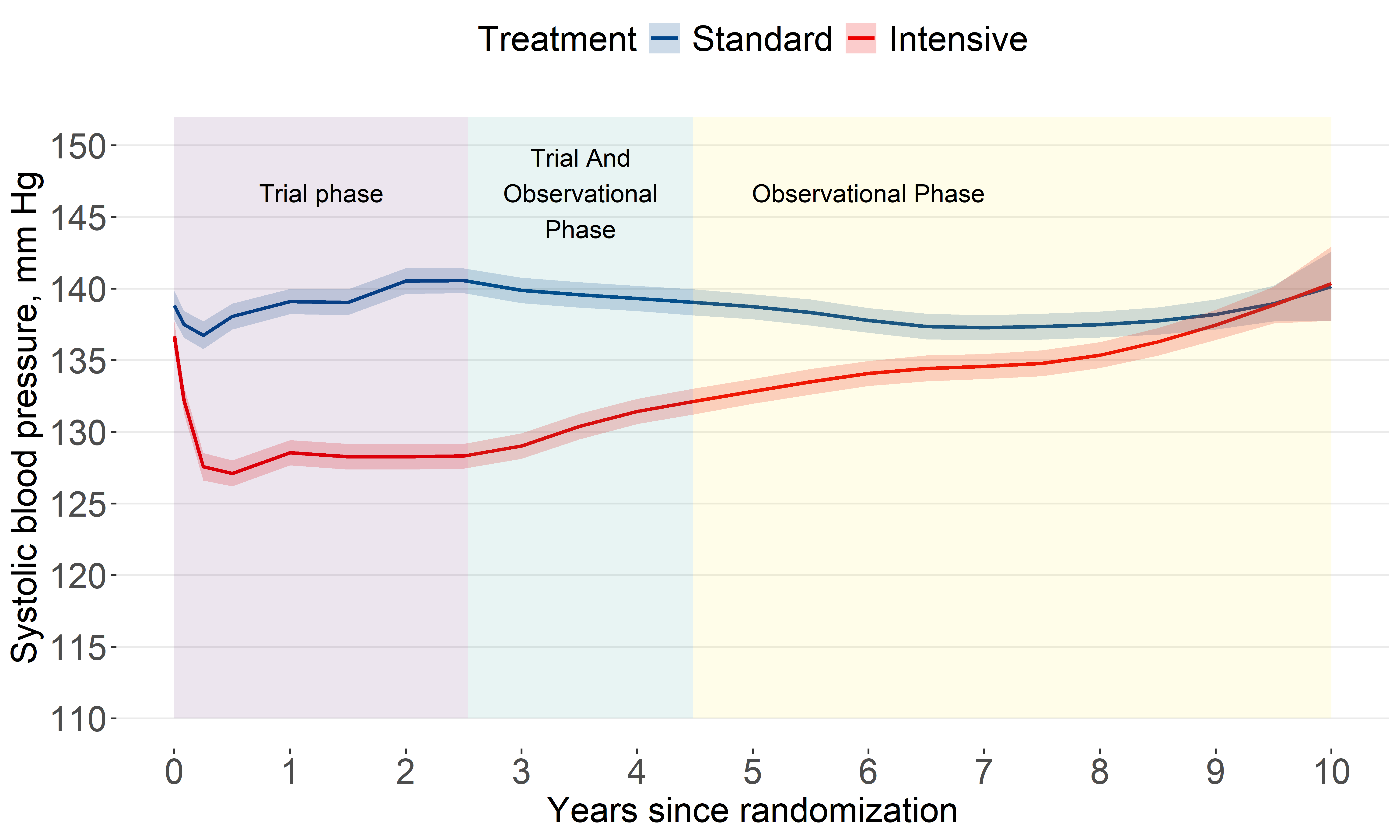
Among 2944 trial participants,3 post-trial SBP levels were analyzed (Drawz et al. 2020).
Systolic BP levels
SBP levels among the intensive group increased after the trial.
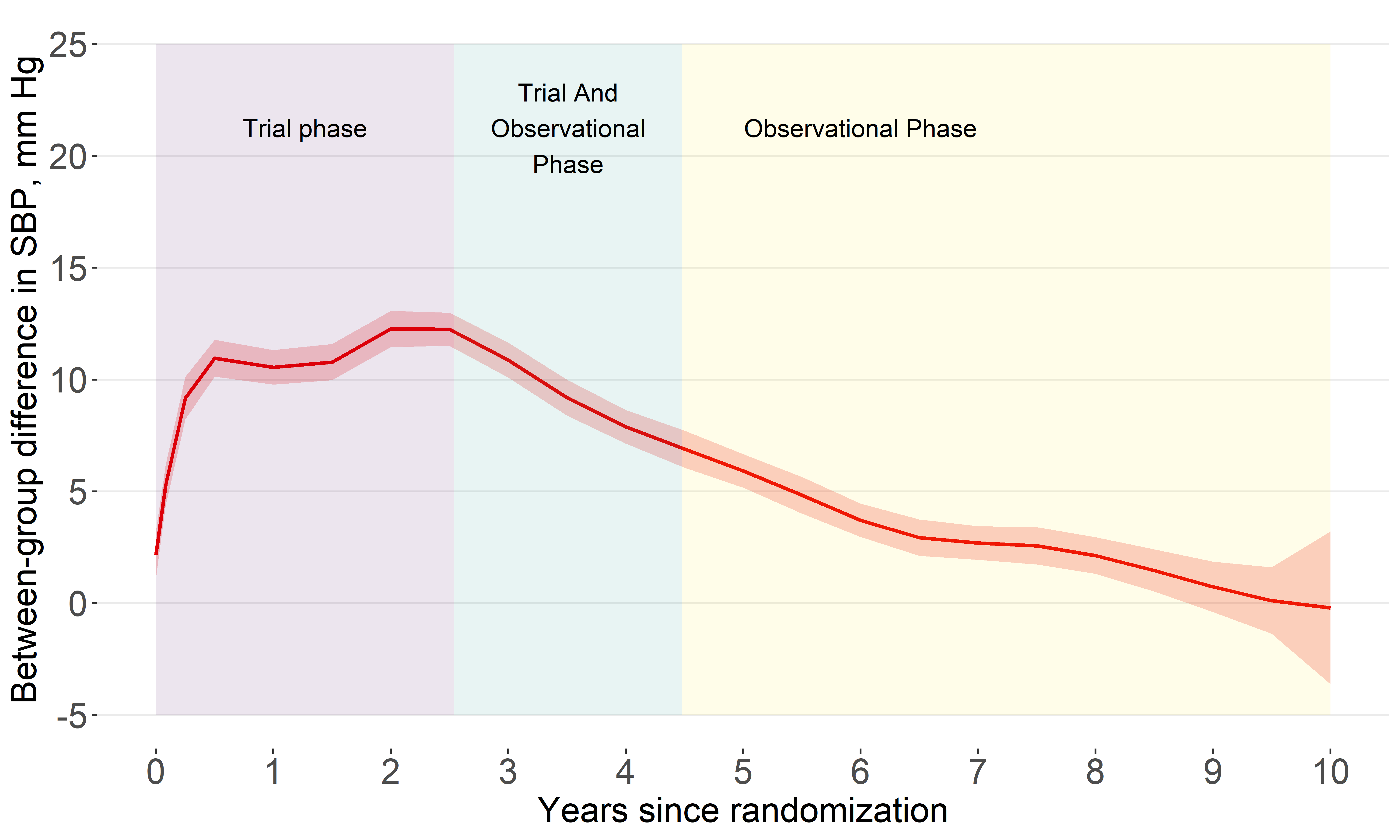
Systolic BP difference
By year 10, the estimated difference was about 0
All-cause mortality (2016-2020)
Our original analysis showed the benefit for all-cause mortality attenuated quickly
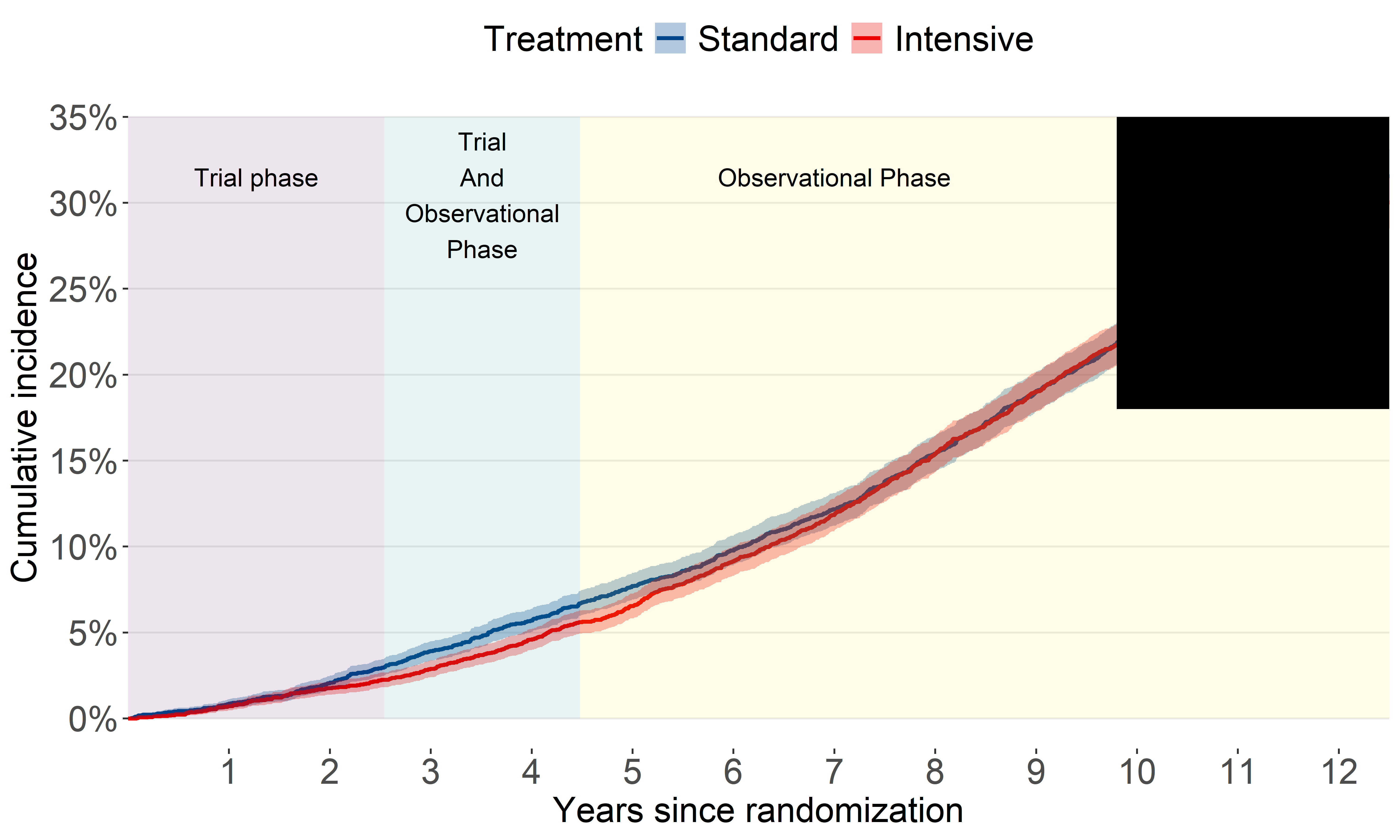
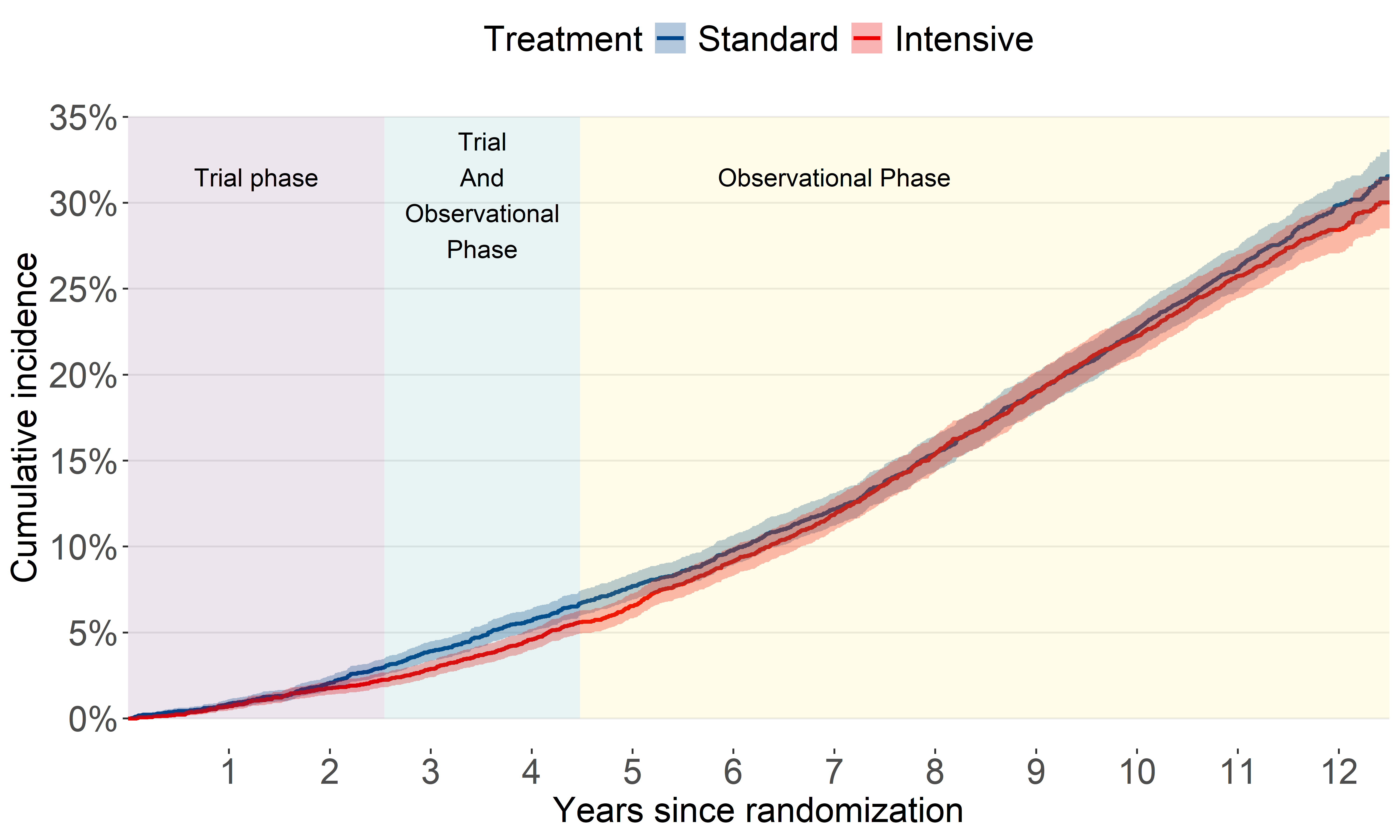
All-cause mortality (2016-2023)
This update shows an unexpected separation after several years of overlap
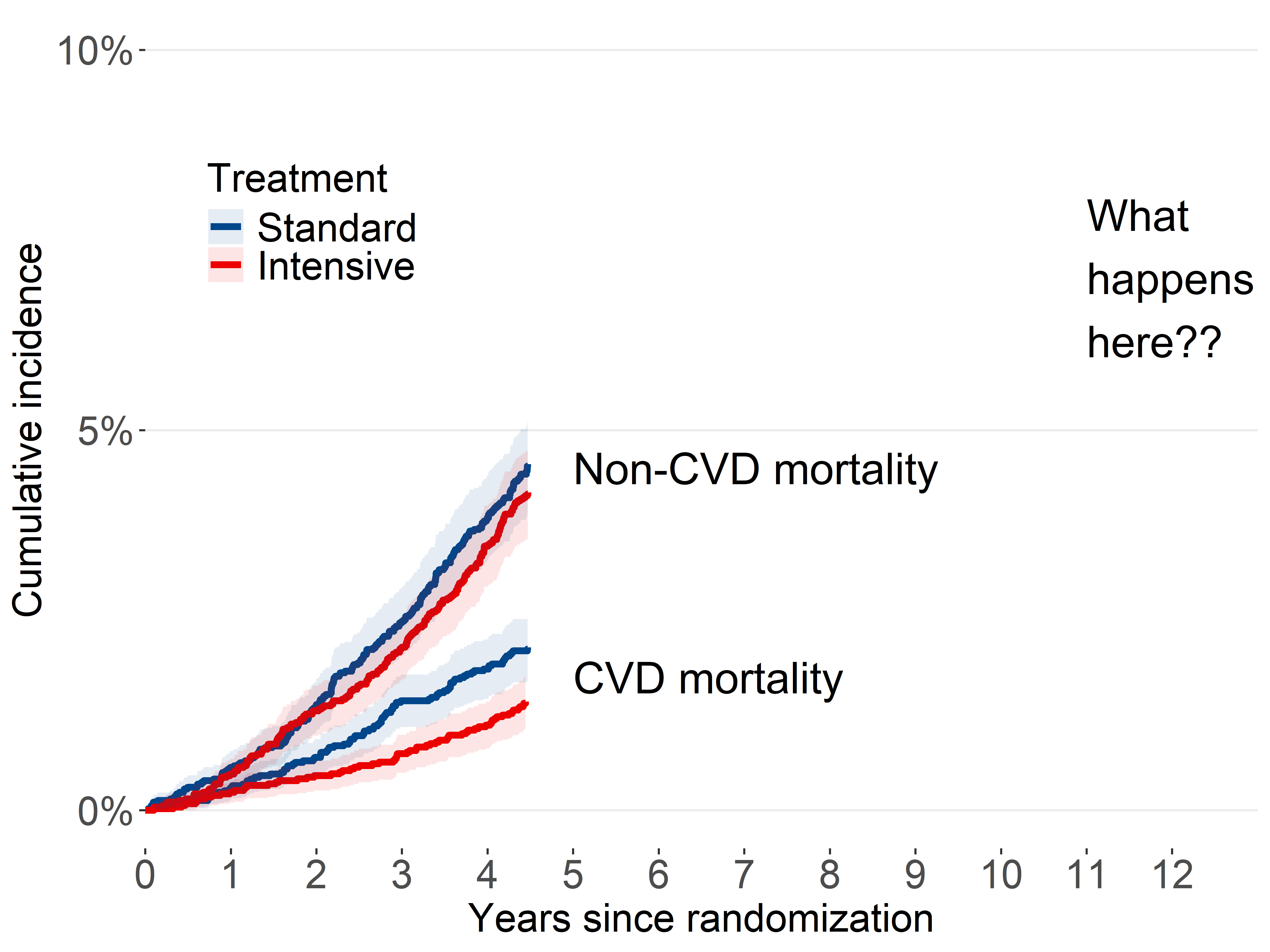
CVD mortality (2016-2020)
Our original analysis showed benefit for CVD mortality attenuated.
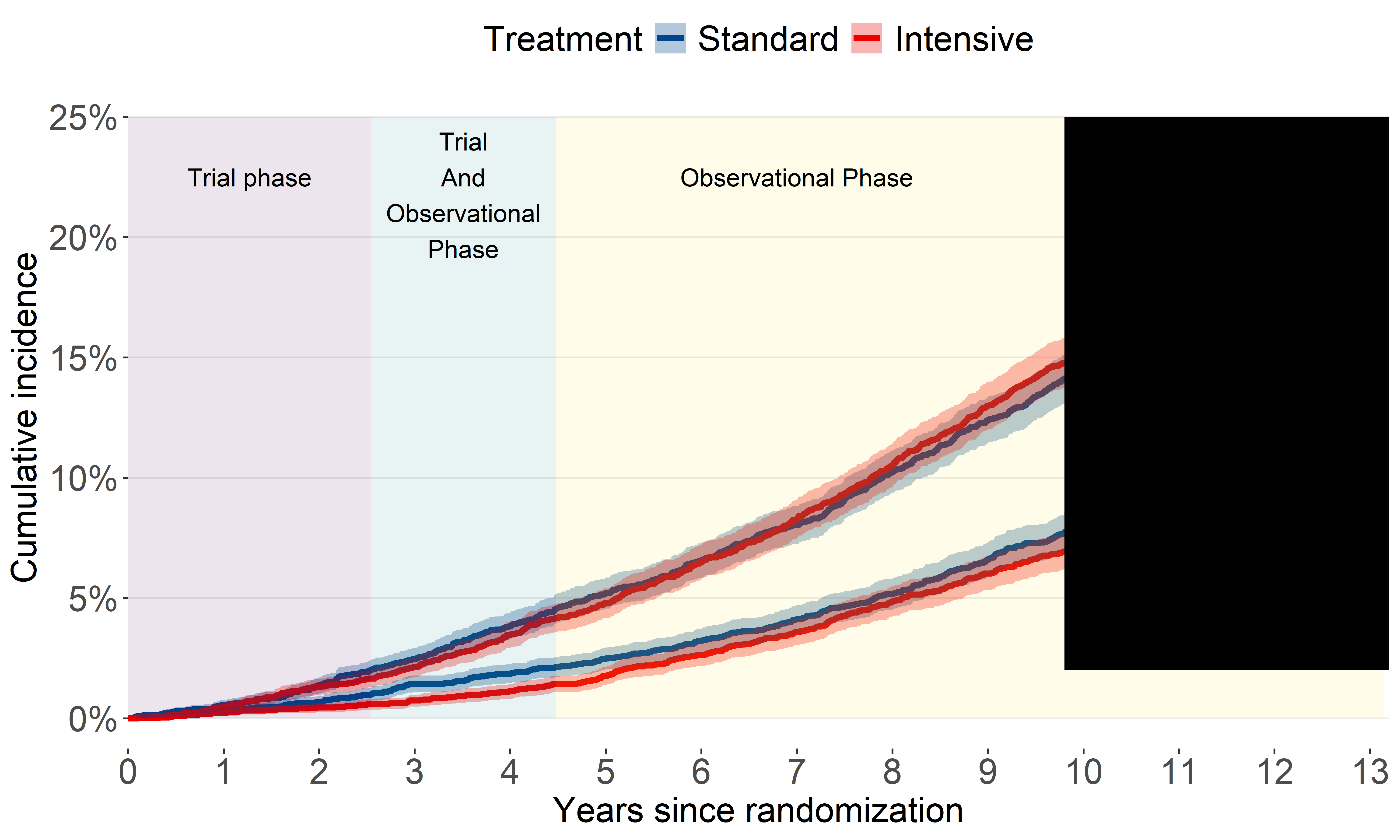
CVD mortality (2016-2023)
A bit of a head-scratcher.
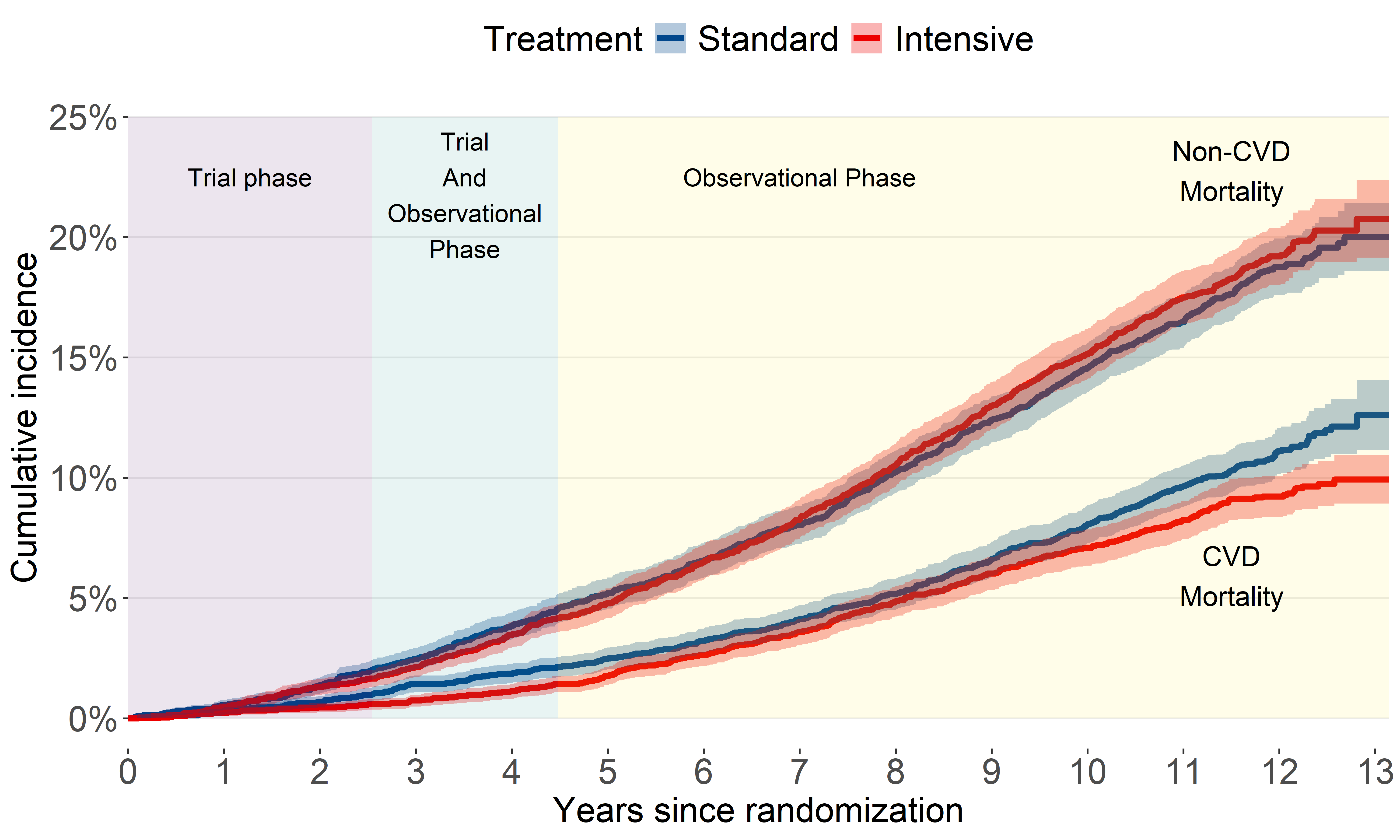
How did we analyze longer term follow-up?
assumed treatment group differences would not be constant over time.
split each participant’s follow-up time into non-overlapping trial and observational phases
estimated regression coefficients for intensive treatment separately during each phase.
All-cause mortalty (time-split analysis)
CVD mortalty (time-split analysis)
Footnotes
Deaths were treated as confirmed if they were a Class 1 match, or a Class 2, 3, or 4 match with a probabilistic score above cutoffs recommended by the NDI.
Cardiovascular mortality for NDI-based follow-up used the NDI Plus System, which automatically identifies underlying causes of death from death certificates, including conversion to International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes. We defined CVD mortality as any death containing the ICD-10 codes of I00 to I99
We identified 3074 participants with 3 or more electronic health record reports of outpatient blood pressure measurements during the trial. After excluding 130 participants without electronic health record data following July 2016 (ie, conclusion of the trial), a total of 2944 patients were included for the ancillary blood pressure analysis.